
Международный эндокринологический журнал Том 21, №7, 2025
Вернуться к номеру
Поширеність захворювань гастродуоденальної ділянки в пацієнтів із тиреоїдною дисфункцією
Авторы: M.A. Derbak, V.V. Timashev, O.T. Hanych, V.V. Svistak, Ye.О. Dankanych
State Higher Educational Institution “Uzhhorod National University”, Uzhhorod, Ukraine
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
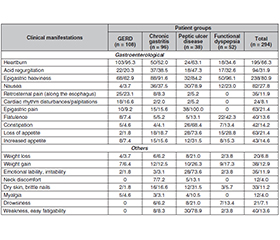
Актуальність. Функціональний стан органів травної системи залежить від складних нейрогуморальних регуляторних механізмів. Зважаючи на здатність гормонів щитоподібної залози (ЩЗ) впливати на гастроінтестинальний гомеостаз, необхідно оцінювати функціональний стан залози та її роль у розвитку різних захворювань шлунково-кишкового тракту. Мета: вивчити частоту основних захворювань травної системи (гастроезофагеальний рефлюкс, виразкова хвороба, гастрит та функціональна диспепсія) у пацієнтів із дисфункцією щитоподібної залози. Матеріали та методи. У дослідження включені 294 хворі з порушеннями функціонального стану ЩЗ. Медикаментозний еутиреоз на тлі прийому препаратів левотироксину зареєстровано у 196 (66,7 %) осіб, у 24 (8,2 %) відзначали неповну компенсацію гіпофункції ЩЗ препаратами левотироксину, оскільки середнє значення тиреотропного гормону (ТТГ) становило 5,42 ± 0,55 мМО/мл та були наявні клінічні симптоми. Гіпотиреоз із рівнем ТТГ від 6,0 до 10,0 мМО/мл діагностовано в 35 (11,9 %) хворих, а рівні > 10,0 мМО/мл зареєстровані у 18 (6,1 %) осіб. Гіпертиреоз спостерігався у 21 з 294 пацієнтів (7,1 %). Підвищення рівнів антитиреоїдних антитіл більше ніж удвічі виявлено в 70 (23,8 %) випадках. Результати. Гастроентерологічну симптоматику відзначено у 81,6 % (240/294) осіб із дисфункцією ЩЗ, вона характеризувалася печією у 66,3 % (195/294) пацієнтів, відчуттям важкості в епігастральній ділянці — у 80,9 % (238/294), погіршенням апетиту — у 21,4 % (63/294), відрижкою — у 31,9 % (94/294), нудотою — у 27,9 % (82/294), блюванням — в 11,9 % (35/294). На метеоризм скаржилися 13,6 % (40/294) обстежених, схильність до запорів — 14,3 % (42/294), біль по ходу стравоходу — 11,9 % (35/294) осіб, біль в епігастральній ділянці — 21,4 % (63/294), перебої в роботі серця — 8,2 % (24/294). У 59,5 % (175/294) хворих виявлено Helicobacter pylori. Гастроезофагеальний рефлюкс зареєстровано в 36,7 % (108/294) пацієнтів, у 31,3 % (92/294) — функціональну диспепсію. Хронічний гастрит діагностовано у 32,6 % (96/294) осіб, а виразкову хворобу — у 12,9 % (38/294). Висновки. Встановлено, що в пацієнтів із гіпотиреозом частіше реєструють гастроезофагеальний рефлюкс та функціональну диспепсію (відповідно 16,7 та 13,5 %), в осіб із медикаментозним еутиреозом — функціональну диспепсію (23,0 %), а при гіпертиреозі — виразкову хворобу (15,7 %). У подальших дослідженнях необхідно оцінити взаємозв’язки між рівнями тиреоїдних гормонів, гастрину й пепсиногенів та з’ясувати вплив гормонів ЩЗ на моторику стравоходу.
Background. The functional state of the digestive system depends on complex neurohumoral regulatory mechanisms. Given the ability of thyroid hormones to influence gastrointestinal homeostasis, it is essential to assess the functional state of the thyroid gland and its role in the development of various gastrointestinal diseases. The aim of the research was to investigate the prevalence of major digestive system disorders (gastroesophageal reflux disease, peptic ulcer disease, gastritis, and functional dyspepsia) in patients with impaired thyroid function. Materials and methods. The study included 294 patients with thyroid dysfunction. Among them, drug-induced euthyroidism maintained with levothyroxine therapy was observed in 196 patients (66.7 %). In 24 individuals (8.2 %), incomplete compensation of thyroid hypofunction with levothyroxine was noted, since the mean thyroid-stimulating hormone (TSH) level was 5.42 ± 0.55 mIU/mL and clinical symptoms were present. Hypothyroidism with TSH levels ranging from 6.0 to 10.0 mIU/mL was found in 35 patients (11.9 %), while TSH levels > 10.0 mIU/mL were registered in 18 (6.1 %). Hyperthyroidism was observed in 21 out of 294 patients (7.1 %). Elevated antithyroid antibody levels (more than twofold above the reference range) were detected in 70 patients (23.8 %). Results. Gastroenterological symptoms among individuals with thyroid dysfunction were identified in 81.6 % (240/294) of patients and were characterized by heartburn in 66.3 % (195/294), a sensation of heaviness in the epigastric region in 80.9 % (238/294), loss of appetite in 21.4 % (63/294), belching in 31.9 % (94/294), nausea in 27.9 % (82/294), and vomiting in 11.9 % (35/294). Flatulence was reported by 13.6 % (40/294), constipation by 14.3 % (42/294), pain along the esophagus by 11.9 % (35/294), epigastric pain by 21.4 % (63/294), and palpitations by 8.2 % (24/294) people. Helicobacter pylori infection was detected in 59.5 % (175/294) of patients. Gastroesophageal reflux disease was diagnosed in 36.7 % (108/294), functional dyspepsia in 31.3 % (92/294), chronic gastritis in 32.6 % (96/294), and peptic ulcer disease in 12.9 % (38/294) of patients. Conclusions. It was found that patients with hypothyroidism more frequently presented with gastroesophageal reflux disease and functional dyspepsia (16.7 and 13.5 %, respectively), those with drug-induced euthyroidism were more likely to develop functional dyspepsia (23.0 %), while patients with hyperthyroidism more commonly had peptic ulcer disease (15.7 %). Further studies should evaluate the relationships between thyroid hormone, gastrin, and pepsinogen levels, as well as clarify the influence of thyroid hormones on esophageal motility.
щитоподібна залоза; гіпотиреоз; гіпертиреоз; еутиреоз; гастроезофагеальний рефлюкс; хронічний гастрит; функціональна диспепсія; виразкова хвороба
thyroid gland; hypothyroidism; hyperthyroidism; euthyroidism; gastroesophageal reflux disease; chronic gastritis; functional dyspepsia; peptic ulcer disease
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Stepanov Y, Skirda I, Petishko O. Digestive system diseases: the actual problem of clinical medicine. Gastroenterology. 2021;53(1):1-6. doi: 10.22141/2308-2097.53.1.2019.163450 (in Ukrainian).
- Bychkov MA, Yakhnytska MM. Gastroesophageal reflux di–sease: a modern view on the problem. Bukovinian Medical Herald. 2019;3(91):118-122. doi: 10.24061/2413-0737.xxiv.3.91.2019.71 (in Ukrainian).
- Tuerk E, Doss S, Polsley K. Peptic ulcer disease. Prim Care. 2023;50(3):351-362. doi: 10.1016/j.pop.2023.03.003.
- Yegen BC. Lifestyle and peptic ulcer disease. Curr Pharm Des. 2018;24(18):2034-2040. doi: 10.2174/1381612824666180510092303.
- Xu GM, Hu MX, Li SY, Ran X, Zhang H, Ding XF. Thyroid disorders and gastrointestinal dysmotility: an old association. Front Physiol. 2024;15:1389113. doi: 10.3389/fphys.2024.1389113.
- Sui X, Jiang S, Zhang H, Wu F, Wang H, et al. The influence of extended fasting on thyroid hormone: local and differentiated regulatory mechanisms. Front Endocrinol (Lausanne). 2024;15:1443051. doi: 10.3389/fendo.2024.1443051.
- Paschou SA, Bletsa E, Stampouloglou PK, Tsigkou V, Valatsou A, et al. Thyroid disorders and cardiovascular manifestations: an update. Endocrine. 2022;75(3):672-683. doi: 10.1007/s12020-022-02982-4.
- Wittekind DA, Kratzsch J, Mergl R, Baber R, Witte V, et al. Free triiodothyronine (T3) is negatively associated with fasting ghrelin serum levels in a population sample of euthyroid subjects. J Endocrinol Invest. 2021;44(12):2655-2664. doi: 10.1007/s40618-021-01578-5.
- Namulema J, Nansunga M, Kato CD, Kalange M, Olaleye SB. Thyroid hormones increase stomach goblet cell numbers and mucin expression during indomethacin induced ulcer healing in Wistar rats. Thyroid Res. 2018;11:6. doi: 10.1186/s13044-018-0050-0.
- Shim S, Ryu HS, Oh HJ, Kim YS. Thyrotoxic vomiting: a case report and possible mechanisms. J Neurogastroenterol Motil. 2010;16(4):428-432. doi: 10.5056/jnm.2010.16.4.428.
- Lee JSG, Brown IE, Semrad AM, Zeki AA. Getting around the gut: a unique management challenge of thyroid storm precipitated by amphetamine-associated duodenal ischaemia leading to compromised enteric absorption. BMJ Case Rep. 2021;14(8):e238889. doi: 10.1136/bcr-2020-238889.
- Pankiv V. Coexistence of accompanying autoimmune di–seases in adolescents with autoimmune thyroiditis. Child’s Health. 2024;19(7):429-433. doi: 10.22141/2224-0551.19.7.2024.1754.
- Hussein S, Alblooshi N, Kandakurti P, Osman H, Mostafa A, et al. Serum TSH, FT3, FT4, and fasting blood glucose levels to investigate the association between thyroid dysfunction and type 2 diabetes mellitus. Georgian Med News. 2025;362:209-213.
- Zhu S, Wang Y, Liu H, Wei W, Tu Y, et al. Thyroxine affects lipopolysaccharide-induced macrophage differentiation and myocardial cell apoptosis via the NF-κB p65 pathway both in vitro and in vivo. Mediators Inflamm. 2019;2019:2098972. doi: 10.1155/2019/2098972.
- Dore MP, Fanciulli G, Manca A, Pes GM. Association of Helicobacter pylori infection with autoimmune thyroid disease in the female sex. J Clin Med. 2023;12(15):5150. doi: 10.3390/jcm12155150.
- Figura N, Di Cairano G, Moretti E, Iacoponi F, Santucci A, et al. Helicobacter pylori infection and autoimmune thyroid disea–ses: the role of virulent strains. Antibiotics (Basel). 2019;9(1):12. doi: 10.3390/antibiotics9010012.
- Hedegaard H, Johnson RL, Garnett MF, Thomas KE. The 2020 International Classification of Diseases, 10th Revision, Clinical Modification Injury Diagnosis Framework for categorizing injuries by body region and nature of injury. Natl Health Stat Rep. 2020;150:1-27.
- Malfertheiner P, Megraud F, O’Morain CA, Gisbert JP, Kuipers EJ, et al.; European Helicobacter and Microbiota Study Group and Consensus Panel. Management of Helicobacter pylori infection — the Maastricht V/Florence Consensus Report. Gut. 2017;66(1):6-30. doi: 10.1136/gutjnl-2016-312288.
- Drossman DA, Hasler WL. Rome IV functional GI disorders: disorders of gut-brain interaction. Gastroenterology. 2016;150(6):1257-1261. doi: 10.1053/j.gastro.2016.03.035.
- Kamada T, Satoh K, Itoh T, Ito M, Iwamoto J, Okimoto T, Kanno T, et al. Evidence-based clinical practice guidelines for peptic ulcer disease 2020. J Gastroenterol. 2021;56(4):303-322. doi: 10.1007/s00535-021-01769-0.
- Laine L, Barkun AN, Saltzman JR, Martel M, Leontiadis GI. ACG clinical guideline: upper gastrointestinal and ulcer bleeding. Am J Gastroenterol. 2021;116(5):899-917. doi: 10.14309/ajg.0000000000001245.
- Chernobrovy VV. Gastroduodenal diseases: nosologic and age-sex pecularity of the express-gastro-pH-monitoring indexes. Bulletin of Scientific Research. 2007;4(49):47-50. Available from: http://nbuv.gov.ua/UJRN/vndt_2007_4(49)__23.
- İlhan M, Arabaci E, Turgut S, Karaman O, Danalioglu A, Tasan E. Esophagus motility in overt hypothyroidism. J Endocrinol Invest. 2014;37(7):639-644. doi: 10.1007/s40618-014-0085-6.
- Nakazawa N, Sohda M, Ogata K, et al. Thyroid hormone activated upper gastrointestinal motility without mediating gastrointestinal hormones in conscious dogs. Sci Rep. 2021;11:9975. doi: 10.1038/s41598-021-89378-y.
- Gunsar F, Yilmaz S, Bor S, Kumanlioğlu K, Cetinkalp S, et al. Effect of hypo- and hyperthyroidism on gastric myoelectrical activity. Dig Dis Sci. 2003;48(4):706-712. doi: 10.1023/a:1022876423487.
- Nogami M, Constantine S, Sai S. Neurological and gastrointestinal symptoms as an initial presentation of pediatric thyroid storm: report of three cases. J Pediatr Endocrinol Metab. 2021;34(9):1197-1200. doi: 10.1515/jpem-2021-0219.
- Adeniyi OS, Emikpe BO, Olaleye SB. Accelerated gastric ulcer healing in thyroxine-treated rats: roles of gastric acid, mucus, and inflammatory response. Can J Physiol Pharmacol. 2018;96(6):597-602. doi: 10.1139/cjpp-2017-0399.
- Arin RM, Gorostidi A, Navarro-Imaz H, Rueda Y, Fresnedo O, Ochoa B. Adenosine: direct and indirect actions on gastric acid secretion. Front Physiol. 2017;8:737. doi: 10.3389/fphys.2017.00737.
- Yaylali O, Kirac S, Yilmaz M, Akin F, Yuksel D, et al. Does hypothyroidism affect gastrointestinal motility? Gastroenterol Res Pract. 2009;2009:529802. doi: 10.1155/2009/529802.