
Журнал «Медицина неотложных состояний» Том 21, №7, 2025
Вернуться к номеру
Прогностичне використання цифрового інструменту для оцінки ризику болю та реабілітаційного навантаження в пацієнтів після ампутації: проспективне спостережне дослідження
Авторы: A. Popelnukha (1, 2), D.V. Dmytriiev (1–3)
(1) - Vinnytsia National Pirogov Memorial Medical University, Vinnytsia, Ukraine
(2) - Center for Pain Management and Rehabilitation “Prometei”, Vinnytsia, Ukraine
(3) - Center for Thermal Trauma and Reconstructive Surgery, Vinnytsia Regional Clinical Hospital named after N.I. Pirogov, Vinnytsia, Ukraine
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
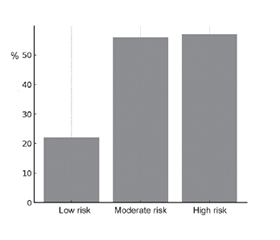
Актуальність. Біль після ампутації та складність реабілітації є поширеними проблемами, які впливають на функціональні результати, особливо в молодих пацієнтів із травматичними ампутаціями. Раннє виявлення осіб групи високого ризику сприяє вчасному втручанню. Матеріали та методи. У цьому проспективному спостережному дослідженні взяли участь 76 пацієнтів (середній вік — 34,1 року; 85 % — чоловіки) з нещодавно проведеними травматичними ампутаціями великих сегментів кінцівок. Оцінку виконували із застосуванням цифрової платформи Protesys протягом трьох тижнів після операції. За допомогою цього інструмента збирали дані про стан рани, інтенсивність болю, стан кукси та психосоціальні ризики (включно з аналізом за шкалою PHQ-9 та індексом катастрофізації болю). Пацієнтів спостерігали протягом трьох місяців. Основним результатом була наявність значущого болю (NRS ≥ 4) або неможливість користуватися протезом ≥ 4 години на добу. Результати. Через три місяці у 36,8 % пацієнтів зберігався середньотяжкий залишковий або фантомний біль. У 15,3 % спостерігали інфекції кукси протягом першого місяця, що вірогідно асоціювалося з хронічним болем (p < 0,01). Лише 60 % учасників могли користуватися протезом ≥ 4 год/добу. Продемонстровано високу точність системи Protesys щодо прогнозування негативних результатів (AUC = 0,82). Багатофакторний аналіз виявив незалежні предиктори, як-от початкова інтенсивність болю (OR 2,1; 95% CI 1,4–3,2), інфекція (OR 3,4; 95% CI 1,7–6,8) та високі показники катастрофізації (OR 1,8; 95% CI 1,1–2,9). У пацієнтів із високим ризиком показники болю або невдалої реабілітації були вдвічі вищими, ніж у групі низького ризику (57 проти 22 %). Висновки. Цифрова платформа Protesys ефективно стратифікує осіб після ампутації за ризиком болю та складністю реабілітації. Її використання на ранньому етапі клінічного обстеження дозволяє своєчасно виявити пацієнтів, які потребують цільового знеболювання, догляду за раною та психологічної підтримки, що сприяє поліпшенню довгострокових результатів відновлення.
Background. Post-amputation pain and rehabilitation difficulty are common challenges that affect functional outcomes, especially in young individuals with traumatic amputations. Early identification of patients at risk allows for proactive intervention. Materials and methods. In this prospective observational study, 76 patients (mean age 34.1 years, 85 % male) with recent traumatic major limb amputations were assessed using the Protesys platform within three weeks post-surgery. The tool collected data on wound status, pain intensity, stump condition, and psychosocial risk (including PHQ-9 and PCS). Patients were followed for three months. The primary outcome was significant pain (NRS ≥ 4) or inability to wear a prosthesis ≥ 4 hours/day. Logistic regression and ROC curve analysis were used to assess predictive accuracy. Results. At three months, 36.8 % of patients experienced moderate-to-severe residual or phantom pain. A total of 15.3 % developed stump infections within the first month, which was significantly associated with persistent pain (p < 0.01). Only 60 % of participants were able to use a prosthesis ≥ 4 hours/day. Protesys scores demonstrated strong predictive accuracy for poor outcomes (AUC = 0.82). Multivariate analysis identified initial pain intensity (OR 2.1, 95% CI 1.4–3.2), infection (OR 3.4, 95% CI 1.7–6.8), and high catastrophizing scores (OR 1.8, 95% CI 1.1–2.9) as independent predictors. Patients categorized as high-risk by digital soft had more than double the rate of pain or rehabilitation failure compared to low-risk patients (57 vs. 22 %). Conclusions. The digital soft tool effectively stratifies post-amputation patients by risk of pain and rehabilitation difficulty. Its integration into early clinical evaluation enables timely identification of patients who may benefit from targeted pain management, wound care, and psychological support, ultimately improving long-term recovery trajectories.
ампутація; прогнозування болю; реабілітація; цифрове здоров’я; фантомний біль; травматичне ушкодження
amputation; pain prediction; rehabilitation; digital health; phantom limb pain; traumatic injury
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Dmytriiev D, Garland EL. Chronic pain during 60 days of war: the impact of the Russian war on Ukrainian patients. J Public Health (Berl). 2024. doi: 10.1007/s10389-024-02243-w.
- Bergauer L, Braun J, Roche TR, et al. Avatar-based patient monitoring improves information transfer, diagnostic confidence and reduces perceived workload in intensive care units: computer-based, multicentre comparison study. Sci Rep. 2023;13:5908. doi: 10.1038/s41598-023-33027-z.
- Tscholl DW, et al. Using an animated patient avatar to improve perception of vital sign information by anaesthesia professionals. Br J Anaesth. 2018;121(3):662-671. doi: 10.1016/j.bja.2018.04.024.
- Battle C, Baker E, Dmytriiev D. Predictors of chronic pain, chronic opioid use and neuropathic pain in Ukrainian military patients with isolated thoracic injuries sustained during the Russia-Ukraine conflict: a single-centre prospective observational study. Eur J Trauma Emerg Surg. 2025;51:237. doi: 10.1007/s00068-025-02914-7.
- Tscholl DW, Weiss M, Handschin L, et al. User perceptions of avatar-based patient monitoring: a mixed qualitative and quantitative study. BMC Anesthesiol. 2018;18:188. doi: 10.1186/s12871-018-0650-1.
- Garot O, Rssler J, Pfarr J, et al. Avatar-based versus conventional vital sign display in a central monitor for monitoring multiple patients: a multicenter computer-based laboratory study. BMC Med Inform Decis Mak. 2020;20:26. doi: 10.1186/s12911-020-1032-4.
- Roche TR, et al. Avatar-based patient monitoring in critical anaesthesia events: a randomised high-fidelity simulation study. Br J Anaesth. 2021;126(5):1046-1054. doi: 10.1016/j.bja.2021.01.015.
- Dobrovanov O, Dmytriiev D, Prochotsky A, Vidiscak M, Furkova K. Pain in COVID-19: quis est culpa? Electron J Gen Med. 2023;20(1):em435. doi: 10.29333/ejgm/12672.
- Wung SF. Human factors and technology in the ICU. Crit Care Nurs Clin North Am. 2018;30(2). doi: 10.1016/j.cnc.2018.03.001.
- Waller RG, Wright MC, Segall N, et al. Novel displays of patient information in critical care settings: a systematic review. J Am Med Inform Assoc. 2019;26(5):479-489. doi: 10.1093/jamia/ocy193.
- Schulz CM, Burden A, Posner KL, et al. Frequency and type of situational awareness errors contributing to death and brain damage: a closed claims analysis. Anesthesiology. 2017;127(2):326-337. doi: 10.1097/aln.0000000000001661.
- Dobrovanov O, Dmytriiev D, Prochotsky A, Vidiscak M, Furkova K. Chronic pain in post-COVID syndrome. Bratisl Med J. 2023;124(2):97-103. doi: 10.4149/bll_2023_014.
- Ksenchyna K, Dmytriiev D, Volanskyi K, Ksenchyn O, Na–zarchuk O. Early post-trauma wound microbiota and its association with pain outcomes and mental health in combat-related extremity injuries: a prospective analysis. Front Pain Res. 2025;6. doi: 10.3389/fpain.2025.1564994.
- Alowais SA, Alghamdi SS, Alsuhebany N, et al. Revolutio–nizing healthcare: the role of artificial intelligence in clinical practice. BMC Med Educ. 2023;23:689. doi: 10.1186/s12909-023-04698-z.
- Buch VH, Ahmed I, Maruthappu M. Artificial intelligence in medicine: current trends and future possibilities. Br J Gen Pract. 2018;68(668):143-144. doi: 10.3399/bjgp18x695213.
- Cabral BP, Braga LAM, Conte Filho CG, Penteado B, Freire de Castro Silva SL, et al. Future use of AI in diagnostic medicine: 2-wave cross-sectional survey study. J Med Internet Res. 2025;27:e53892. doi: 10.2196/53892.
- Salomon I, Olivier S. Artificial intelligence in medicine: advantages and disadvantages for today and the future. Int J Surg Open. 2024;62(4):471-473. doi: 10.1097/io9.0000000000000133.
- Popelnukha A, Dmytriiev D. Rapid pain assessment tool avatar self-pain report: a new objective method for adequate pain diagnosis? Pilot study. Emerg Med. 2025;21(4):394-397. doi: 10.22141/2224-0586.21.4.2025.1887.
- Peir AM, Margargit C, Llerena A. Drug-drug interactions: things to do in pain management. Drug Metab Pers Ther. 2018;33(1):1-2. doi: 10.1515/dmpt-2017-0029.
- Hermann M, Carstens N, Kvinge L, et al. Polypharmacy and potential drug-drug interactions in home-dwelling older people: a cross-sectional study. J Multidiscip Healthc. 2021;14:589-597. doi: 10.2147/jmdh.s297423.
- Pirnejad H, Amiri P, Niazkhani Z, et al. Preventing potential drug-drug interactions through alerting decision support systems: a clinical context-based methodology. Int J Med Inform. 2019;127:18-26. doi: 10.1016/j.ijmedinf.2019.04.006.
- Emery MA, Akil H. Endogenous opioids at the intersection of opioid addiction, pain, and depression: the search for a precision medicine approach. Annu Rev Neurosci. 2020;43:355-374. doi: 10.1146/annurev-neuro-110719-095912.
- Compton WM, Valentino RJ, DuPont RL. Polysubstance use in the U.S. opioid crisis. Mol Psychiatry. 2021;26(1):41-50. doi: 10.1038/s41380-020-00949-3.
- Fang T, Zhang X, Hao W, et al. The status and prescription patterns of opioid utilization in a large comprehensive teaching hospital in China according to the anatomical therapeutic chemical classification/defined daily dose methodology. Front Psychiatry. 2022;13:913640. doi: 10.3389/fpsyt.2022.913640.