
Журнал «Боль. Суставы. Позвоночник» Том 15, №3, 2025
Вернуться к номеру
Біль у нижній частині спини у будівельників: перехресне дослідження
Авторы: V. Moodley, J.D. Pillay
Durban University of Technology, Durban, South Africa
Рубрики: Ревматология, Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
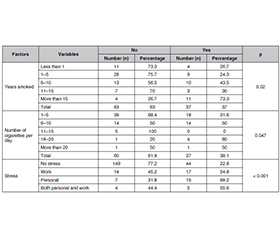
Актуальність. Біль у нижній частині спини (БНС), пов’язаний із професійною діяльністю, привертає все більше уваги, особливо щодо його негативного впливу на продуктивність праці та інвалідність. Будівельні робітники (БР) мають одну з найбільш фізично тяжких професій, що робить їх надзвичайно чутливими до БНС. Мета: вивчити поширеність БНС та визначити окремі фактори ризику серед БР у муніципалітеті Етеквіні (Квазулу-Натал, Південна Африка). Матеріали та методи. Перехресне опитування проведено серед БР за місцем роботи у відповідних компаніях. Анкета включала розділи щодо демографічних показників, способу життя, професійних факторів ризику та історії БНС. Для аналізу даних використовували програму IBM SPSS версії 28. Статистично значущі відмінності між групами підтверджували з використанням показника р < 0,05. Було проаналізовано поширеність БНС на момент обстеження та протягом останніх 6 міс. Результати. Поширеність БНС на момент обстеження та протягом останніх 6 міс. становила відповідно 16,8 та 26,2 %. За результатами аналізу виявлено, що 36,6 % курців, які палили на момент обстеження, мали БНС, а серед тих, хто курить понад 15 років, цей показник становив 73,3 %. Важливим фактором БНС був стрес: 54,8 % пацієнтів, які зазнали стресу внаслідок роботи, і 68,2 % осіб зі стресом, пов’язаним з особистими причинами, повідомляли про БНС на відміну від 22,8 % обстежених, які не відчували стресу. Монтажники риштувань продемонстрували більшу поширеність БНС (50 %), ніж різноробочі (43,2 %), монтажники (33,3 %) та муляри (30,5 %). Висновки. БНС продовжує залишатися значним тягарем для здоров’я БР, впливаючи на їхню повсякденну діяльність і спричиняючи інвалідність. Тому необхідна спільна стратегія втручання між медичними працівниками та будівельною галуззю. Це зменшить прогули, стрес, поліпшить продуктивність та обмеження активності.
Background. Occupational-related lower back pain (LBP) has received growing attention, especially regarding its effect on work productivity and disability. Construction workers (CWs) are involved in one of the most physically demanding occupations, making them exceedingly susceptible to LBP. The objective was to determine LBP’s prevalence and identify selected risk factors among CWs within the eThekwini Municipality in KwaZulu-Natal, South Africa. Materials and methods. A cross-sectional survey was conducted on 256 CWs, and questionnaires were provided to participants at their respective companies. The questionnaire included sections on demographics, lifestyle, occupational risk factors, and LBP history. IBM SPSS version 28 was used to analyze the data. A p-value of < 0.05 was used to indicate statistical significance. Both point prevalence (occurrence of LBP at the time of the survey) and period prevalence (occurrence of LBP over the past six months) were analyzed. Results. The point and period prevalences were 16.8 and 26.2 %, respectively. The results indicated that 36.6 % of current smokers reported LBP, with a higher incidence of 73.3 % among those smoking for over 15 years. Stress emerged as a significant factor; 54.8 % of subjects experiencing work-related stress and 68.2 % under personal stress reported LBP, contrasted with only 22.8 % of those experiencing no stress. Scaffolders exhibited a higher LBP prevalence (50 %) than general workers (43.2 %), erectors (33.3 %), and bricklayers (30.5 %). Conclusions. LBP continues to be a significant health burden for CWs, impacting their daily activities and causing disability. Therefore, a joint intervention strategy between health professionals and the construction industry is required. This will reduce absenteeism, stress, decreased productivity and activity limitations.
біль у попереку; будівельники; спосіб життя; професійні фактори; Південна Африка
low back pain; construction workers; lifestyle; occupational factors; South Africa
Introduction
Materials and methods
Results
/24.jpg)
/24_2.jpg)
/25.jpg)
Discussion
Conclusions
/27.jpg)
/28.jpg)
/29.jpg)
- Wu A, March L, Zheng X, et al. Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the Global Burden of Disease Study 2017. Ann Transl Med. 2020 Mar;8(6):299. doi: 10.21037/atm.2020.02.175.
- Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017 Feb 18;389(10070):736-747. doi: 10.1016/S0140-6736(16)30970-9.
- Gopalakrishnan S, Kumar PM. Risk Factors of Morbidity among Construction Workers: A review. IJCMPH. 2020;7(11):4664-4671. doi: 10.18203/2394-6040.ijcmph20204772.
- Lee YC, Hong X, Man SS. Prevalence and Associated Factors of Work-Related Musculoskeletal Disorders Symptoms among Construction Workers: A Cross-Sectional Study in South China. Int J Environ Res Public Health. 2023 Mar 6;20(5):4653. doi: 10.3390/ijerph20054653.
- Anton D, Bray M, Hess JA, Weeks DL, Kincl LD, Vaughan A. Prevalence of work-related musculoskeletal pain in masonry apprentices. Ergonomics. 2020 Sep;63(9):1194-1202. doi: 10.1080/00140139.2020.1772380.
- Bento TPF, Genebra CVDS, Maciel NM, Cornelio GP, Simeão SFAP, Vitta A. Low back pain and some associated factors: is there any difference between genders? Braz J Phys Ther. 2020 Jan-Feb;24(1):79-87. doi: 10.1016/j.bjpt.2019.01.012.
- Cezar-Vaz MR, Bonow CA, Xavier DM, et al. Prevalence of Low Back Pain and Dorsalgia and Associated Factors among Casual Dockworkers. Int J Environ Res Public Health. 2018 Oct 20;15(10):2310. doi: 10.3390/ijerph15102310.
- Alghadir A, Anwer S. Prevalence of musculoskeletal pain in construction workers in Saudi Arabia. ScientificWorldJournal. 2015;2015:529873. doi: 10.1155/2015/529873.
- Machado Susseret N, Briceno-Ayala L, Radon K. Prevalence of low back pain in migrant construction workers in Mar del Plata, Argentina. Am J Ind Med. 2019 Sep;62(9):777-782. doi: 10.1002/ajim.23016.
- Morris LD, Daniels KJ, Ganguli B, Louw QA. An update on the prevalence of low back pain in Africa: a systematic review and meta-analyses. BMC Musculoskelet Disord. 2018 Jun 21;19(1):196. doi: 10.1186/s12891-018-2075-x.
- Khumalo K, Haffejee F. Prevalence and associated risk factors of low back pain among users of a primary health care clinic serving semi-urban and rural settlements in KwaZulu-Natal, South Africa. Afr Health Sci. 2022 Jun;22(2):592-601. doi: 10.4314/ahs.v22i2.68.
- Kahere M, Hlongwa M, Ginindza TG. A Scoping Review on the Epidemiology of Chronic Low Back Pain among Adults in Sub-Saharan Africa. Int J Environ Res Public Health. 2022 Mar 3;19(5):2964. doi: 10.3390/ijerph19052964.
- Doualla M, Aminde J, Aminde LN, et al. Factors influencing disability in patients with chronic low back pain attending a tertiary hospital in sub-Saharan Africa. BMC Musculoskelet Disord. 2019 Jan 15;20(1):25. doi: 10.1186/s12891-019-2403-9.
- Othman N, Jiar YK. Low Back Pain Risk Assessment for Construction Industry Personnel. Indian J Public Health Res Dev. 2019;10(4):1399-1404.
- Adhikari B, Ghimire A, Jha N, et al. Factors associated with low back pain among construction workers in Nepal: A cross-sectional study. PLoS One. 2021 Jun 1;16(6):e0252564. doi: 10.1371/journal.pone.0252564.
- Dlungwane T, Voce A, Knight S. Prevalence and factors associated with low back pain among nurses at a regional hospital in KwaZulu-Natal, South Africa. Health SA. 2018 May 29;23:1082. doi: 10.4102/hsag.v23i0.1082.
- Hoy D, Brooks P, Blyth F, Buchbinder R. The Epidemiology of low back pain. Best Pract Res Clin Rheumatol. 2010 Dec;24(6):769-781. doi: 10.1016/j.berh.2010.10.002.
- Manchikanti L, Singh V, Falco FJ, Benyamin RM, Hirsch JA. Epidemiology of low back pain in adults. Neuromodulation. 2014 Oct;17(Suppl 2):3-10. doi: 10.1111/ner.12018.
- Walker BF. The prevalence of low back pain: a systematic review of the literature from 1966 to 1998. J Spinal Disord. 2000 Jun;13(3):205-217. doi: 10.1097/00002517-200006000-00003.
- Meucci RD, Fassa AG, Faria NMX. Prevalence of chronic low back pain: systematic review. Rev Saude Publica. 2015;49:1. doi: 10.1590/S0034-8910.2015049005874.
- Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012 Jun;64(6):2028-2037. doi: 10.1002/art.34347.
- Kwon JW, Ha JW, Lee TS, Moon SH, Lee HM, Park Y. Comparison of the Prevalence of Low Back Pain and Related Spinal Diseases among Smokers and Nonsmokers: Using Korean National Health Insurance Database. Clin Orthop Surg. 2020 Jun;12(2):200-208. doi: 10.4055/cios19095.
- Xu HR, Zhang YH, Ngo TL, Yang QH, Du SH, Wang XQ. Association between smoking and incident back pain: A prospective cohort study with 438 510 participants. J Glob Health. 2023 Nov 22;13:04152. doi: 10.7189/jogh.13.04152.
- Lv Z, Cui J, Zhang J. Smoking, alcohol and coffee consumption and risk of low back pain: a Mendelian randomization study. Eur Spine J. 2022 Nov;31(11):2913-2919. doi: 10.1007/s00586-022-07389-3.
- Pirouzi S, Ghanbari A, Moslemi Haghighi F, Ghafarinejad F, Pouya F, Motiallah T. The prevalence of musculoskeletal pain in male cigarette smoking students at Shiraz University of Medical Sciences, Iran. Addict Health. 2011;3(3-4):125-129.
- Smuck M, Schneider BJ, Ehsanian R, Martin E, Kao MJ. Smoking Is Associated with Pain in All Body Regions, with Greatest Influence on Spinal Pain. Pain Med. 2020 Sep 1;21(9):1759-1768. doi: 10.1093/pm/pnz224.
- Yang QH, Zhang YH, Du SH, Wang YC, Wang XQ. Association between Smoking and Pain, Functional Disability, Anxiety and Depression in Patients With Chronic Low Back Pain. Int J Public Health. 2023 Mar 7;68:1605583. doi: 10.3389/ijph.2023.1605583.
- Chen N, Fong DYT, Wong JYH. Health and economic burden of low back pain and rheumatoid arthritis attributable to smoking in 192 countries and territories in 2019. Addiction. 2024 Apr;119(4):677-685. doi: 10.1111/add.16404.
- Scott JR, Hassett AL, Schrepf AD, et al. Moderate Alcohol Consumption Is Associated with Reduced Pain and Fibromyalgia Symptoms in Chronic Pain Patients. Pain Med. 2018 Dec 1;19(12):2515-2527. doi: 10.1093/pm/pny032.
- Yang H, Haldeman S. Behavior-Related Factors Associated with Low Back Pain in the US Adult Population. Spine (Phila Pa 1976). 2018 Jan 1;43(1):28-34. doi: 10.1097/BRS.0000000000001665.
- Karimi R, Mallah N, Nedjat S, Beasley MJ, Takkouche B. Association between alcohol consumption and chronic pain: a systematic review and meta-analysis. Br J Anaesth. 2022 Sep;129(3):355-365. doi: 10.1016/j.bja.2022.03.010.
- Hung HY, Chien WC, Chung CH, et al. Patients with alcohol use disorder increase pain and analgesics use: A nationwide population-based cohort study. Drug Alcohol Depend. 2021 Dec 1;229(Pt A):109102. doi: 10.1016/j.drugalcdep.2021.109102.
- LaRowe LR, Powers JM, Garey L, Rogers AH, Zvolensky MJ, Ditre JW. Pain-related anxiety, sex, and co-use of alcohol and prescription opioids among adults with chronic low back pain. Drug Alcohol Depend. 2020 Sep 1;214:108171. doi: 10.1016/j.drugalcdep.2020.108171.
- Robins MT, Heinricher MM, Ryabinin AE. From Pleasure to Pain, and Back Again: The Intricate Relationship Between Alcohol and Nociception. Alcohol Alcohol. 2019 Dec 1;54(6):625-638. doi: 10.1093/alcalc/agz067.
- Alzahrani H, Mackey M, Stamatakis E, Zadro JR, Shirley D. The association between physical activity and low back pain: a systematic review and meta-analysis of observational studies. Sci Rep. 2019 Jun 3;9(1):8244. doi: 10.1038/s41598-019-44664-8.
- Lemes ÍR, Pinto RZ, Turi Lynch BC, et al. The Association Between Leisure-time Physical Activity, Sedentary Behavior, and Low Back Pain: A Cross-sectional Analysis in Primary Care Settings. Spine (Phila Pa 1976). 2021 May 1;46(9):596-602. doi: 10.1097/BRS.0000000000003996.
- Kędra A, Plandowska M, Kędra P, Czaprowski D. Physical activity and low back pain in children and adolescents: a systematic review. Eur Spine J. 2021 Apr;30(4):946-956. doi: 10.1007/s00586-020-06575-5.
- Martins MDDS, Lemes ÍR, Esposito E, et al. Association between Domain-Specific Physical Activity and Chronic Low Back Pain in Community-Dwelling Older Adults: A Cross-Sectional Study. J Aging Phys Act. 2023 Mar 16;31(5):798-805. doi: 10.1123/japa.2022-0279.
- Heuch I, Heuch I, Hagen K, Zwart JA. Physical activity level at work and risk of chronic low back pain: A follow-up in the Nord-Trøndelag Health Study. PLoS One. 2017 Apr 10;12(4):e0175086. doi: 10.1371/journal.pone.0175086.
- Balling M, Holmberg T, Petersen CB, Aadahl M, Meyrowitsch DW, Tolstrup JS. Total sitting time, leisure time physical activity and risk of hospitalization due to low back pain: The Danish Health Examination Survey cohort 2007-2008. Scand J Public Health. 2019 Feb;47(1):45-52. doi: 10.1177/1403494818758843.
- Choi S, Nah S, Jang HD, Moon JE, Han S. Association between chronic low back pain and degree of stress: a nationwide cross-sectional study. Sci Rep. 2021 Jul 15;11(1):14549. doi: 10.1038/s41598-021-94001-1.
- Tsuboi Y, Ueda Y, Naruse F, Ono R. The Association Between Perceived Stress and Low Back Pain Among Eldercare Workers in Japan. J Occup Environ Med. 2017 Aug;59(8):765-767. doi: 10.1097/JOM.0000000000001062.
- Vinstrup J, Jakobsen MD, Andersen LL. Perceived Stress and Low-Back Pain among Healthcare Workers: A Multi-Center Prospective Cohort Study. Front Public Health. 2020 Aug 11;8:297. doi: 10.3389/fpubh.2020.00297.
- Chung JWY, So HCF, Yan VCM, et al. A Survey of Work-Related Pain Prevalence Among Construction Workers in Hong Kong: A Case-Control Study. Int J Environ Res Public Health. 2019 Apr 18;16(8):1404. doi: 10.3390/ijerph16081404.
- Ben-Ami N, Korn L. Associations between backache and stress among undergraduate students. J Am Coll Health. 2020 Jan;68(1):61-67. doi: 10.1080/07448481.2018.1515753.
- Wippert PM, Puerto Valencia L, Drießlein D. Stress and Pain. Predictive (Neuro)Pattern Identification for Chronic Back Pain: A Longitudinal Observational Study. Front Med (Lausanne). 2022 May 10;9:828954. doi: 10.3389/fmed.2022.828954.
- Mierswa T, Kellmann M. Differences in low back pain occurrence over a 6-month period between four recovery-stress groups. Work. 2017;58(2):193-202. doi: 10.3233/WOR-172618.
- Anwer S, Li H, Antwi-Afari MF, Wong AYL. Associations between physical or psychosocial risk factors and work-related musculoskeletal disorders in construction workers based on literature in the last 20 years: a systematic review. Int J Ind Ergon. 2021 May;83:103113. doi: 10.1016/j.ergon.2021.103113.
- Yin Z, Caldas C. Scaffolding in industrial construction projects: current practices, issues, and potential solutions. Int J Constr Manag. 2022;22(13):2554-2563. doi: 10.1080/15623599.2020.1808562.
- Antwi-Afari MF, Li H, Chan AHS, et al. A science mapping-based review of work-related musculoskeletal disorders among construction workers. J Safety Res. 2023 Jun;85:114-128. doi: 10.1016/j.jsr.2023.01.011.