
Международный эндокринологический журнал Том 21, №5, 2025
Вернуться к номеру
Вплив системних супутніх захворювань та цукрового діабету на виживання при раку голови та шиї: когортне дослідження
Авторы: P.I. Mykhailiuk (1), V.V. Boiko (2), I.A. Dmytrenko (2), A.Ye. Kryzhanivska (1)
(1) - Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine
(2) - Precarpathian Clinical Oncology Center, Ivano-Frankivsk, Ukraine
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
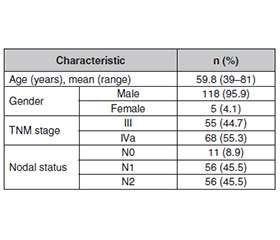
Актуальність. Прогноз у пацієнтів із місцево-поширеним раком голови та шиї часто ускладнюється системними супутніми захворюваннями. Специфічний вплив метаболічних розладів, зокрема цукрового діабету, на результати лікування залишається критичним міждисциплінарним питанням. Метаболічні розлади, як-от цукровий діабет, все частіше визнаються вагомими модифікаторами прогресування раку й толерантності до лікування. Гіперглікемія може погіршувати імунну функцію та призводити до росту пухлини, а також збільшувати ризик післяопераційних ускладнень. Тому розуміння взаємодії між супутніми ендокринними захворюваннями й онкологічними наслідками має вирішальне значення для розробки інтегрованих стратегій ведення пацієнтів. Мета: аналіз впливу навантаження супутніх захворювань, кількісно визначеного за допомогою індексу коморбідності Чарльсона (ІКЧ), на толерантність до лікування, рівень ускладнень та загальну виживаність пацієнтів із місцево-поширеним гіпофарингеальним раком III–IVa стадії. Матеріали та методи. Було проведено ретроспективний аналіз медичних даних 123 пацієнтів, які лікувалися між 2013 і 2024 роками. Вони були стратифіковані в групи ризику на основі ІКЧ. Первинні кінцеві точки — загальна виживаність та частота фарингошкірних нориць. Для первинного аналізу когорту розділено на три клінічно значущі групи ризику на основі розрахованого ІКЧ: низький ризик (ІКЧ 0–1; n = 54), помірний (ІКЧ 2–3; n = 41) та високий (ІКЧ ≥ 4; n = 28). Результати. Вищий ІКЧ корелював із гіршими результатами лікування (p < 0,001). Примітно, що наявність існуючого цукрового діабету була пов’язана з вищою частотою тяжких післяопераційних ускладнень. У багатовимірному аналізі високий ІКЧ (≥ 4) був найсильнішим незалежним предиктором смертності (коефіцієнт ризику 3,15; p < 0,001), перевищуючи стадію TNM. Висновки. Загальний вплив супутніх захворювань є ключовим прогностичним фактором при раку голови та шиї. Ці результати підкреслюють важливість ретельного метаболічного контролю та міждисциплінарного підходу за участю ендокринологів у веденні пацієнтів із раком голови та шиї для поліпшення хірургічних результатів та загальної виживаності.
Background. The prognosis for patients with locally advanced head and neck cancer is often complicated by systemic comorbidities. The specific impact of metabolic disorders, particularly diabetes mellitus, on treatment outcomes remains a critical interdisciplinary issue. Particularly, metabolic disorders such as diabetes mellitus are increasingly recognized as significant modifiers of cancer progression and treatment tolerance. Hyperglycemia can impair immune function and promote tumor growth, while also increasing the risk of postoperative complications. Therefore, understanding the interplay between endocrinological comorbidities and oncological outcomes is crucial for developing integrated patient management strategies. Aim of the study was to analyze the impact of the comorbidity burden, quantified by the Charlson Comorbidity Index (CCI), on treatment tolerance, complication rates, and overall survival in patients with stage III–IVa locally advanced hypopharyngeal cancer. Materials and methods. A retrospective analysis of medical data from 123 patients treated between 2013 and 2024 was performed. They were stratified into risk groups based on the CCI. Primary endpoints were overall survival and the incidence of pharyngocutaneous fistula. For the primary analysis, the cohort was stratified into three clinically relevant risk groups based on the calculated CCI scores: low-risk (CCI 0–1; n = 54), moderate-risk (CCI 2–3; n = 41), and high-risk (CCI ≥ 4; n = 28). Results. A higher CCI score strongly correlated with worse outcomes (p < 0.001). Notably, the presence of pre-existing diabetes mellitus was associated with a higher incidence of severe postoperative complications. In multivariate analysis, a high CCI score (≥ 4) was the strongest independent predictor of mortality (hazard ratio 3.15; p < 0.001), surpassing TNM stage. Conclusions. The overall comorbidity burden is a key prognostic factor in locally advanced head and neck cancer. These findings underscore the importance of meticulous metabolic control and a multidisciplinary approach involving endocrinologists in the management of head and neck cancer patients to improve surgical outcomes and overall survival.
гіпофарингеальний рак; цукровий діабет; супутні захворювання; індекс коморбідності Чарльсона; результат лікування; виживання; фарингошкірна нориця
hypopharyngeal cancer; diabetes mellitus; comorbidity; Charlson Comorbidity Index; treatment outcome; survival; pharyngocutaneous fistula
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Kwon DI, Miles BA; Education Committee of the American Head and Neck Society (AHNS). Hypopharyngeal carcinoma: Do you know your guidelines? Head Neck. 2019;41(3):569-576. doi: 10.1002/hed.24752.
- Ferrari M, Mularoni F, Smussi D, et al.; Consensus Group for Laryngeal Preservation. International consensus on laryngeal pre–servation strategies in laryngeal and hypopharyngeal cancer. Lancet Oncol. 2025;26(5):e264-e281. doi: 10.1016/s1470-2045(25)00020-8.
- Katano A, Yamashita H, Saito Y, Kobayashi K. The role of upfront neck dissection in definitive radiotherapy for locally advanced hypopharyngeal squamous cell carcinoma: A single-center retrospective analysis. Head Neck. 2024;46(11):2815-2823. doi: 10.1002/hed.27839.
- Stordeur S, Schillemans V, Savoye I, et al. Comorbidity in head and neck cancer: Is it associated with therapeutic delay, post-treatment mortality and survival in a population-based study? Oral Oncol. 2020;102:104561. doi: 10.1016/j.oraloncology.2019.104561.
- Mykhailiuk PI, Hirna HA, Kostyshyn ID, et al. Retrospective analysis of radical treatment of patients with stage III–IVa hypopharyngeal cancer. Clinical Oncology. 2025;15(2):1-5. doi: 10.32471/clinicaloncology.2663-466x.34351 (in Ukrainian).
- Wang J, Zhang W, Sun K, et al. Developing a framework for estimating comorbidity burden of inpatient cancer patients based on a case study in China. Glob Health Res Policy. 2025;10(1):13. doi: 10.1186/s41256-025-00411-3.
- Guller M, Cooper DJ, Alkhatib H, et al. Impact of comorbidities on outcomes in patients with advanced head and neck cancer undergoing immunotherapy. Head Neck. 2023;45(11):2789-2797. doi: 10.1002/hed.27502.
- Price JM, Mell LK. Managing patients with head and neck cancer and advanced age or comorbidities. Semin Radiat Oncol. 2025;35(2):197-206. doi: 10.1016/j.semradonc.2025.02.001.
- Datema FR, Ferrier MB, Vergouwe Y, et al. Update and external validation of a head and neck cancer prognostic model. Head Neck. 2013;35(9):1232-1237. doi: 10.1002/hed.23117.
- Kim DH, Kim SW, Hwang SH. Predictive value of risk factors for pharyngocutaneous fistula after total laryngectomy. Laryngoscope. 2023;133(4):742-754. doi: 10.1002/lary.30278.
- Sticker AL, Cannon ST, Russell GB, Waltonen JD. Factors associated with adjuvant treatment delays in patients treated surgically for head and neck cancer. Clin Otolaryngol. 2024;49(4):445-452. doi: 10.1111/coa.14164.
- Alabdullah M, Shaker K, Alomar K, Sardini Z, Hamdan A, Yousef O. Management of pharyngocutaneous fistula following laryng–ectomy with autologous fat graft: A case report and literature review. Int J Surg Case Rep. 2024;120:109781. doi: 10.1016/j.ijscr.2024.109781.
- Marschner SN, Maihöfer C, Späth R, et al. Adjuvant (chemo)radiotherapy for patients with head and neck cancer: Can comorbidity risk scores predict outcome? Strahlenther Onkol. 2024;200(12):1025-1037. doi: 10.1007/s00066-024-02282-y.
- Kang HW, Kim SM, Kim WT, et al.; KORCC (KOrean Renal Cell Carcinoma) Group. The age-adjusted Charlson comorbi–dity index as a predictor of overall survival of surgically treated non-me–tastatic clear cell renal cell carcinoma. J Cancer Res Clin Oncol. 2020;146(1):187-196. doi: 10.1007/s00432-019-03042-7.
- Hendrickx JJ, Mennega T, Uppelschoten JM, Leemans CR. Changes in multidisciplinary team decisions in a high volume head and neck oncological center following those made in its preferred partner. Front Oncol. 2023;13:1205224. doi: 10.3389/fonc.2023.1205224.
- Kunz V, Gänzle M, Dietz A, Wichmann G. Frailty, nutritional status and prehabilitation in head and neck oncology. Laryngorhinooto–logie. 2025;104(6):384-397. doi: 10.1055/a-2473-3880 (in German).
- Haehl E, Rühle A, Spohn S, et al. Patterns-of-care analysis for radiotherapy of elderly head-and-neck cancer patients: A trinational survey in Germany, Austria and Switzerland. Front Oncol. 2022;11:723716. doi: 10.3389/fonc.2021.723716.
- Noor A, Gibb C, Boase S, Hodge JC, Krishnan S, Foreman A. Frailty in geriatric head and neck cancer: A contemporary review. Laryngoscope. 2018;128(12):E416-E424. doi: 10.1002/lary.27339.
- Membreno PV, Luttrell JB, Mamidala MP, et al. Outcomes of primary radiotherapy with or without chemotherapy for advanced oral cavity squamous cell carcinoma: Systematic review. Head Neck. 2021;43(10):3165-3176. doi: 10.1002/hed.26779.
- Orlandi E, Bossi P. Toward personalized cancer care for elderly head and neck cancer patients. Int J Radiat Oncol Biol Phys. 2017;98(4):965-966. doi: 10.1016/j.ijrobp.2016.11.001.