
Международный эндокринологический журнал Том 20, №4, 2024
Вернуться к номеру
Зв’язок холекальциферолу і паратгормону з метаболічними порушеннями у хворих на артеріальну гіпертензію
Авторы: M.M. Semіaniv (1), L.P. Sydorchuk (1), Yu.M. Yarynych (1), Sai Praveen Daruvuri(2), S.B. Semenenko (1), O.I. Sydorchuk (3)
(1) - Bukovinian State Medical University, Chernivtsi, Ukraine
(2) - St. Mary’s General Hospital, Passaic, New Jersey, USA
(3) - Bogomolets National Medical University, Kyiv, Ukraine
Рубрики: Эндокринология
Разделы: Справочник специалиста
Версия для печати
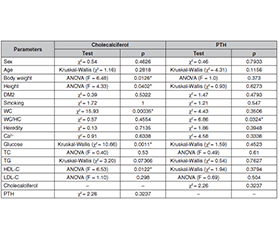
Актуальність. Есенціальна артеріальна гіпертензія (ЕАГ) — складне, багатофакторне й полігенне захворювання. Незважаючи на ефективні заходи з контролю та модифікації традиційних чинників ризику, його ступінь залишається значним. Метою дослідження було оцінити зміни клінічних показників і проаналізувати взаємозв’язок паратгормону, холекальциферолу з антропометричними, метаболічними параметрами у хворих на ЕАГ. Матеріали та методи. У дослідження типу «випадок — контроль» було залучено 100 осіб з ЕАГ та ураженням органів-мішеней (друга стадія), помірним, високим, дуже високим серцево-судинним ризиком. Контрольну групу становили 60 здорових осіб, порівнянних за статтю й віком. Критерій Пірсона використовували для визначення зв’язку між параметрами у випадку категоріальних змінних; дисперсійний аналіз (ANOVA) — коли одна зі змінних є категорійною, а інша — числовою (інтервальною); непараметричний критерій Крускала — Уолліса — у випадку ненормального розподілу масиву. Результати. Розвиток і перебіг ЕАГ характеризуються клінічними, гемодинамічними, метаболічними порушеннями, які нелінійно посилюються зі збільшенням тяжкості гіпертензії. Кореляційний аналіз показав прямий зв’язок між масою тіла та співвідношенням окружності талії до окружності стегон (ОТ/ОС) (r = 0,76–0,88; р < 0,001); систолічний артеріальний тиск помірно прямо корелює з ОТ (r = 0,38; р < 0,05); рівень загального холестерину сильно асоційований з умістом холестерину ліпопротеїнів низької щільності (r = 0,93; р < 0,001), рівень холестерину ліпопротеїнів високої щільності (ХС-ЛПВЩ) обернено асоційований з ОТ (r = –0,40; р < 0,05) і вмістом тригліцеридів (r = –0,41; р < 0,001), а концентрація холекальциферолу негативно пов’язана з індексом маси тіла, співвідношенням ОТ/ОС (r = –0,41/–0,38; р < 0,05). Аналіз ANOVA підтвердив зв’язок холекальциферолу плазми з масою тіла (F = 6,48; р = 0,013), зростом (F = 4,33; р = 0,04), ОТ (χ2 = 15,93; р < 0,001), рівнем глюкози крові (χ2 = 10,66; р = 0,001) та ХС-ЛПВЩ (F = 6,53; р = 0,012). Установлено вірогідний зв’язок між умістом паратгормону й співвідношенням ОТ/ОС (χ2 = 6,86; р = 0,032). Висновки. У хворих на ЕАГ рівень холекальциферолу в плазмі вірогідно корелює з масою тіла, зростом, ОТ, рівнем глюкози, ХС-ЛПВЩ. Паратгормон має прямий зв’язок зі співвідношенням ОТ/ОС.
Background. Essential hypertension (EH) is a complex, multifactorial and polygenic disease. Despite effective measures for control and modification of traditional risk factors, a significant amount of risk remains. The aim of the study was to evaluate changes in clinical parameters and to analyze the relationship of cholecalciferol, parathyroid hormone with anthropometric, metabolic parameters in patients with EH. Materials and methods. One hundred subjects with EH and target organ damage (stage 2), moderate, high, very high cardiovascular risk were enrolled in case-control study. Control group consisted of 60 healthy subjects matched for sex and age. Pearson’s test was used to determine the relationship between parameters in case of categorical variables; analysis of variance (ANOVA) when one of the variables is categorical and the other is numerical (interval); non-parametric Kruskal-Wallis test in case of abnormal array distribution. Results. Development and course of EH is characterized by clinical, hemodynamic, metabolic abnormalities that are nonlinearly exacerbated with the severity of hypertension. Correlation analysis showed a direct relationship between body weight and waist-to-hip ratio (r = 0.76–0.88; р < 0.001); systolic blood pressure is moderately directly correlated with waist circumference (WC) (r = 0.38; р < 0.05); total cholesterol is strongly associated with low-density lipoprotein cholesterol (r = 0.93; р < 0.001), high-density lipoprotein cholesterol (HDL-C) is inversely associated with WC (r = –0.40; р < 0.05) and triacylglycerol levels (r = –0.41; р < 0.001), and cholecalciferol concentration is negatively marginally associated with body mass index, waist-to-hip ratio (r = –0.41/–0.38; р < 0.05). ANOVA confirmed that plasma cholecalciferol was associated with body weight (F = 6.48; р = 0.013), height (F = 4.33; р = 0.04), WC (χ2 = 15.93; р < 0.001), blood glucose (χ2 = 10.66; р = 0.001) and HDL-С (F = 6.53; р = 0.012). Reliable relationship between parathyroid hormone and waist-to-hip ratio was found (χ2 = 6.86; р = 0.032). Conclusions. In EH patients, plasma cholecalciferol significantly correlates with body weight, height, WC, glucose level, HDL-С. Parathyroid hormone has a significant and direct relationship with waist-to-hip ratio.
есенціальна артеріальна гіпертензія; холекальциферол; паратгормон; метаболічні показники; зв’язок
essential hypertension; cholecalciferol; parathyroid hormone; metabolic parameters; relationship
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur Heart J. 2018;39:3021-3104. doi: 10.1093/eurheartj/ehy339.
- World Health Organization Hypertension (accessed on 30 August 2021). Available from: https://www.who.int/westernpacific/health-topics/hypertension.
- Zhou B, Carrillo-Larco RM, Danaei G, Riley LM, Paciorek CJ, et al. Worldwide Trends in Hypertension Prevalence and Progress in Treatment and Control from 1990 to 2019: A Pooled Analysis of 1201 Population-Representative Studies with 104 Million Participants. Lancet. 2021;398:957-980. doi: 10.1016/S0140-6736(21)01330-1.
- Afshin A, Forouzanfar MH, Reitsma MB, Sur P, Estep K, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med 2017;377(1):13-27. doi: 10.1056/NEJMoa1614362.
- Kuwabara M, Kuwabara R, Niwa K, Hisatome I, et al. Diffe–rent Risk for Hypertension, Diabetes, Dyslipidemia, and Hyperuricemia According to Level of Body Mass Index in Japanese and American Subjects. Nutrients. 2018;10(8):1011. doi: 10.3390/nu10081011.
- Vishram JK, Borglykke A, Andreasen AH, Jeppesen J, Ibsen H, et al.; MORGAM Project. Impact of age on the importance of systolic and diastolic blood pressures for stroke risk: the MOnica, Risk, Gene–tics, Archiving, and Monograph (MORGAM) Project. Hypertension. 2012 Nov;60(5):1117-23. doi: 10.1161/HYPERTENSIONAHA.112.201400.
- Ministry of Health of Ukraine. On approval and implementation of medical and technological documents on standardization of medical care for arterial hypertension. Order of the Ministry of Health of Ukraine of 24.05.2012 No. 384. Kyiv: Ministry of Health of Ukraine; 2012. Available from: https://zakon.rada.gov.ua/rada/show/v038428212#Tex.
- Semianiv M, Sydorchuk L, Fedonyuk L, Nebesna Z, Kamyshnyi O, et al. Metabolic and hormonal prognostic markers of essential arterial hypertension considering the genes polymorphism AGTR1 (rs5186) and VDR (rs2228570). Romanian Journal of Diabetes Nutrition and Metabolic Diseases. 2021;28(3):284-291. Available from: https://www.rjdnmd.org/index.php/RJDNMD/article/view/1049.
- Repchuk Y, Sydorchuk LP, Sydorchuk AR, et al. Linkage of blood pressure, obesity and diabetes mellitus with angiotensinogen gene (AGT 704T>C/rs699) polymorphism in hypertensive patients. Bratisl Lek Listy. 2021;122(10):715-720. doi: 10.4149/BLL_2021_114.
- Sydorchuk L, Dzhuryak V, Sydorchuk A, et al. The cytochrome 11B2 aldosterone synthase gene rs1799998 single nucleotide polymorphism determines elevated aldosterone, higher blood pressure, and reduced glomerular filtration, especially in diabetic female patients. Endocrine Regulations. 2020;54(3):217-226. doi: 10.2478/enr-2020-0024.
- Hnizdiukh R, Shmanko V. Gene polymorphism among residents of Ternopil region afflicted with essential arterial hypertension. Medical Scien–ce of Ukraine (MSU). 2021;17(4). doi: 10.32345/2664-4738.4.2021.04.
- Semianiv MM, Sydorchuk LP, Dzhuryak VS, et al. Association of AGTR1 (rs5186), VDR (rs2228570) genes polymorphism with blood pressure elevation in patients with essential arterial hypertension. J Med Life. 2021;14(6):782-789. doi: 10.25122/jml-2021-0018.
- Sydorchuk A, Sydorchuk L, Gutnitska A, et al. The role of NOS3 (rs2070744) and GNB3 (rs5443) genes’ polymorphisms in endothelial dysfunction pathway and carotid intima-media thickness in hypertensive patients. General Physiology and Biophysics. 2023;42(2):179-190. doi: 10.4149/gpb_2022060.
- Ta N, Liu M, Wang Y, Zeng F, Nie F, et al. Association of polymorphisms in endothelial dysfunction-related genes with susceptibility to essential hypertension in elderly Han population in Liaoning province, China. Rev Cardiovasc Med. 2021 Sep 24;22(3):895-901. doi: 10.31083/j.rcm2203096.
- Voroniuk K, Sydorchuk L, Repchuk Yu, Sydorchuk A, Sydor–chuk R, Iftoda O. Novel Genetics and Humoral Prognostic Markers of Left Ventricle Hypertrophy in Hypertensive Patients. Journal of Medical Sciences. 2024 Jan-Feb;44(1):18-25. doi: 10.4103/jmedsci.jmedsci_66_23.
- Semianiv M, Sydorchuk L. Clinical and metabolic parameters, Ca2+, parathormone depending on serum 25(OH)D concentration in hypertensive patients in the West-Ukrainian population. J Educ Health Sport. 2021 Dec 14;11(12):150-7. Available from: https://apcz.umk.pl/JEHS/article/view/36478.
- Tanaka M, Itoh H. Hypertension as a Metabolic Disorder and the Novel Role of the Gut. Curr Hypertens Rep. 2019;21(8):63. doi: 10.1007/s11906-019-0964-5.
- Karadeniz Y, Özpamuk-Karadeniz F, Ahbab S, Ataoğlu E, Can G. Vitamin D Deficiency Is a Potential Risk for Blood Pressure Elevation and the Development of Hypertension. Medicina (Kaunas). 2021 Nov 25;57(12):1297. doi: 10.3390/medicina57121297.
- Argano C, Mirarchi L, Amodeo S, Orlando V, Torres A, Corrao S. The Role of Vitamin D and Its Molecular Bases in Insulin Resistance, Diabetes, Metabolic Syndrome, and Cardiovascular Di–sease: State of the Art. Int J Mol Sci. 2023 Oct 23;24(20):15485. doi: 10.3390/ijms242015485.
- Liu L, Lei J, Zhang L, et al. A multiethnic association analysis of hyperuricaemia with cardiovascular risk in rural and urban areas in Chinese adults. Sci Rep. 2021 Dec 3;11(1):23362. doi: 10.1038/s41598-021-02740-y.
- Liu L, Quang ND, Banu R, et al. Hypertension, blood pressure control and diabetic retinopathy in a large population-based study. PLoS One. 2020 Mar 5;15(3):e0229665. doi: 10.1371/journal.pone.0229665.
- Zhdan V, Volchenko H, Babanina M, et al. The problem of timely diagnosis of primary hyperaldosteronism. Clinical case. International Journal of Endocrinology (Ukraine). 2023;19(6):464-468. doi: 10.22141/2224-0721.19.6.2023.1318.
- Marushchak M, Mazur L, Krynytska I. Insulin receptor substrate-1 gene polymorphism and lipid panel data in type 2 diabetic patients with comorbid obesity and/or essential hypertension. Endocr Regul. 2023;57(1):1-11. doi: 10.2478/enr-2023-0001.