
Международный эндокринологический журнал Том 19, №3, 2023
Вернуться к номеру
Вплив гіпотиреозу на перебіг ішемічної хвороби серця у пацієнтів зі зниженою фракцією викиду лівого шлуночка
Авторы: Кучерява М.В., Маньковський Г.Б.
ДУ «Науково-практичний медичний центр дитячої кардіології та кардіохірургії» МОЗ України,
клініка для дорослих, м. Київ, Україна
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
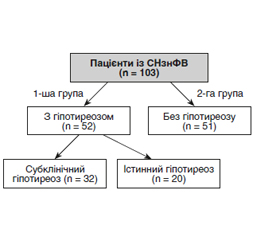
Актуальність. Гормони щитоподібної залози відіграють фундаментальну роль у гомеостазі серцево-судинної системи. Серцево-судинні захворювання є одними з найбільш поширених хвороб у всьому світі, спричинюють чималий відсоток смертності, госпіталізацій та інвалідизації. Мета дослідження: оцінити вплив гіпотиреозу на перебіг атеросклеротичного ураження коронарних артерій та великих серцево-судинних подій у пацієнтів із серцевою недостатністю (СН) зі зниженою фракцією викиду лівого шлуночка після проведення реваскуляризації міокарда за допомогою черезшкірного коронарного втручання (ЧКВ). Матеріали та методи. Проспективне обсерваційне одноцентрове дослідження включало 103 пацієнти з ішемічною кардіоміопатією, серцевою недостатністю зі зниженою фракцією викиду, яким було проведено ЧКВ, з наявним гіпотиреозом і без нього. Результат реваскуляризації оцінено протягом двох років. Критерії включення: пацієнти віком старше від 18 років, з ішемічною хворобою серця, фракцією викиду лівого шлуночка менше ніж 40 %. Результати. Пацієнти з гіпотиреозом мали гірший ліпідний профіль і, як і очікувалося, мали вищий вихідний рівень тиреотропного гормону (ТТГ). За даними ЕхоКГ, у хворих на гіпотиреоз відзначалося потовщення стінок міокарда лівого шлуночка, на що вказує вірогідне підвищення показників розмірів задньої стінки лівого шлуночка (11,40 ± 0,98 мм, р < 0,001). У першій групі пацієнти мали вищі показники маси міокарда як один із критеріїв гіпертрофії лівого шлуночка (172,73 ± 12,72 г/м2, р < 0,001). Після багатофакторного аналізу з використанням регресії пропорційних ризиків Кокса підвищений рівень ТТГ все ще асоціювався зі значно вищими показниками серцево-судинної смертності (ВР 0,85; 95% ДІ 0,75–0,95; р < 0,001), повторного ЧКВ (ВР 0,75; 95% ДІ 0,65–0,85; р < 0,05) та декомпенсації з приводу серцевої недостатності (ВР 0,88; 95% ДІ 0,78–0,96; р < 0,05). Висновки. Гіпотиреоз асоціюється з вищою частотою первинної комбінованої кінцевої точки у вигляді повторного ЧКВ, госпіталізацій з приводу декомпенсації СН та вторинної кінцевої точки — серцево-судинної смертності порівняно з еутиреозом у пацієнтів протягом двох років спостереження. Підтримання адекватного контролю ТТГ у пацієнтів з ІХС та серцевою недостатністю зі зниженою фракцією викиду лівого шлуночка є прогностично важливим для запобігання серцево-судинним подіям.
Background. Thyroid hormones play a fundamental role in the homeostasis of the cardiovascular system. Cardiovascular diseases are among the most common diseases worldwide, causing a significant percentage of mortality, hospitalizations, and disability. The purpose of the study is to evaluate the impact of hypothyroidism on the course of atherosclerotic lesions of coronary arteries and major cardiovascular events in patients with heart failure with reduced left ventricular ejection fraction after myocardial revascularization using percutaneous coronary intervention (PCI). Materials and methods. This prospective observational one-center study included 103 patients with ischemic cardiomyopathy, heart failure with reduced left ventricular ejection fraction, with and without hypothyroidism who underwent PCI. The result of revascularization was evaluated within 2 years. Inclusion criteria: age over 18 years, coronary artery disease, left ventricular ejection fraction less than 40 %. Results. Patients with hypothyroidism had a worse lipid profile and, as expected, a higher baseline thyroid-stimulating hormone (TSH). According to echocardiography, patients with hypothyroidism had thickening of the left ventricular myocardium walls, which is indicated by a probable increase in the dimensions of the left ventricular posterior wall (11.40 ± 0.98 mm; p < 0.001). In the first group, patients had higher myocardial mass indicators as one of the criteria for left ventricular hypertrophy (172.73 ± 12.72 g/m2; p < 0.001). After multivariate analysis using Cox proportional hazards regression, an elevated TSH level was still associated with significantly higher rates of cardiovascular mortality (risk ratio (RR) 0.85; 95% confidence interval (CI) 0.75–0.95; p < 0.001), repeat PCI (RR 0.75; 95% CI 0.65–0.85; p < 0.05) and decompensation due to heart failure (RR 0.88; 95% CI 0.78–0.96; p < 0.05). Conclusions. Hypothyroidism is associated with a higher incidence of the primary composite endpoint of repeat PCI, hospitalizations for decompensated heart failure, and the secondary endpoint of cardiovascular mortality compared to euthyroid patients over two years of follow-up. Maintaining adequate control of TSH in patients with coronary artery disease and heart failure with reduced ejection fraction is prognostically important for preventing cardiovascular events.
гіпотиреоз; ішемічна хвороба серця; серцева недостатність зі зниженою фракцією викиду; атеросклероз коронарних артерій; ремоделювання лівого шлуночка
hypothyroidism; coronary artery disease; heart failure with reduced ejection fraction; atherosclerosis of coronary arteries; left ventricular remodeling
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Von Hafe M., Neves J.S., Vale C., Borges-Canha M., Leite-Moreira A. The impact of thyroid hormone dysfunction on ische–mic heart disease. Endocr. Connect. 2019 May 1. 8(5). R76-R90. doi: 10.1530/EC-19-0096. PMID: 30959486; PMCID: PMC6499922.
- McDonagh T.A., Metra M., Adamo M., Gardner R.S., Baumbach A., Böhm M., Burri H., et al.; ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021 Sep 21. 42(36). 3599-3726. doi: 10.1093/eurheartj/ehab368. Erratum in: Eur. Heart J. 2021 Oct 14. PMID: 34447992.
- Mehran L., Amouzegar A., Rahimabad P.K., Tohidi M., Tahmasebinejad Z., Azizi F. Thyroid function and metabolic syndrome: a population-based thyroid study. Horm. Metab. Res. 2017. 49. 192-200. doi: 10.1055/s-0042-117279.
- Pankiv V.I., Yuzvenko T.Yu., Pankiv I.V. Type 2 diabetes mellitus and subclinical hypothyroidism: focusing on the role of cholecalciferol. Problems of Endocrine Pathology. 2019. 2. 46-51. Doi: 10.21856/j-PEP.2019.2.07.
- Strikić Đula I., Pleić N., Babić Leko M., Gunjača I., Torlak V., Brdar D., et al. Epidemiology of Hypothyroidism, Hyperthyroi–dism and Positive Thyroid Antibodies in the Croatian Population. Bio–logy (Basel). 2022 Mar 2. 11(3). 394. doi: 10.3390/biology11030394. PMID: 35336768; PMCID: PMC8945477.
- Papadopoulou A.M., Bakogiannis N., Skrapari I., Moris D., Bakoyiannis C. Thyroid dysfunction and atherosclerosis: a systematic review. In Vivo. 2020. 34. 3127-36. doi: 10.21873/invivo.12147.
- Abreu I.M., Lau E., de Sousa Pinto B., Carvalho D. Subclinical hypothyroidism: to treat or not to treat, that is the question! A systematic review with meta-analysis on lipid profile. Endocr. Connect. 2017 Apr. 6(3). 188-199. doi: 10.1530/EC-17-0028. Epub 2017 Mar 1. PMID: 28249936; PMCID: PMC5428911.
- Cooper D.S., Biondi B. Subclinical thyroid disease. Lancet. 2012. 379. 1142-54. doi: 10.1016/S0140-6736(11)60276-6.
- Stojković M., Žarković M. Subclinical Thyroid Dysfunction and the Risk of Cardiovascular Disease. Curr. Pharm. Des. 2020. 26(43). 5617-5627. doi: 10.2174/1381612826666201118094747. PMID: 33213317.
- Papadopoulou A.M., Bakogiannis N., Skrapari I., Moris D., Bakoyiannis C. Thyroid Dysfunction and Atherosclerosis: A Systematic Review. In Vivo. 2020 Nov-Dec. 34(6). 3127-3136. doi: 10.21873/invivo.12147. PMID: 33144416; PMCID: PMC7811672.
- Grais I.M., Sowers J.R. Thyroid and the heart. Am. J. Med. 2014 Aug. 127(8). 691-8. doi: 10.1016/j.amjmed.2014.03.009. Epub 2014 Mar 22. PMID: 24662620; PMCID: PMC4318631.
- Alibaz Oner F., Yurdakul S., Oner E., Kubat Uzum A., Erguney M. Evaluation of the effect of L-thyroxin therapy on endothelial functions in patients with subclinical hypothyroidism. Endocrine. 2011 Oct. 40(2). 280-4. doi: 10.1007/s12020-011-9465-2. Epub 2011 Apr 20. PMID: 21505892.
- Pasyechko N.V., Kulchinska V.M., Naumova L. Subclinical hypothyroidism in pregnant women in the iodine deficiency region: to treat or not to treat? International Journal of Endocrinology (Ukraine). 2020. 16. 471-477. DOI: 10.22141/2224-0721.16.6.2020.215385.
- Suh S., Kim D.K. Subclinical Hypothyroidism and Cardiovascular Disease. Endocrinol. Metab. (Seoul). 2015 Sep. 30(3). 246-51. doi: 10.3803/EnM.2015.30.3.246. Epub 2015 Aug 4. PMID: 26248862; PMCID: PMC4595347.
- Rodondi N., den Elzen W.P., Bauer D.C., Cappola A.R., Razvi S., Walsh J.P., Asvold B.O., et al.; Thyroid Studies Collaboration. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA. 2010 Sep 22. 304(12). 1365-74. doi: 10.1001/jama.2010.1361. PMID: 20858880; PMCID: PMC3923470.
- Friberg L., Drvota V., Bjelak A.H., Eggertsen G., Ahnve S. Association between increased levels of reverse triiodothyronine and mortality after acute myocardial infarction. Am. J. Med. 2001 Dec 15. 111(9). 699-703. doi: 10.1016/s0002-9343(01)00980-9. PMID: 11747849.
- Brozaitiene J., Mickuviene N., Podlipskyte A., Burkauskas J., Bunevicius R. Relationship and prognostic importance of thyroid hormone and N-terminal pro-B-Type natriuretic peptide for patients after acute coronary syndromes: a longitudinal observational study. BMC Cardiovasc. Disord. 2016 Feb 18. 16. 45. doi: 10.1186/s12872-016-0226-2. PMID: 26892923; PMCID: PMC4757967.
- Cappola A.R., Desai A.S., Medici M., Cooper L.S., Egan D., Sopko G., Fishman G.I., et al. Thyroid and Cardiovascular Disease Research Agenda for Enhancing Knowledge, Prevention, and Treatment. Circulation. 2019 May 13:10.1161/CIRCULATIONAHA.118.036859. doi: 10.1161/CIRCULATIONAHA.118.036859. Epub ahead of print. PMID: 31081673; PMCID: PMC6851449.
- Ravindran S., Kurian G.A. Addressing the alterations in cerebral ischemia-reperfusion injury on the brain mitochondrial activity: A possible link to cognitive decline. Biochem. Biophys. Res. Commun. 2019 Oct 8. 518(1). 100-106. doi: 10.1016/j.bbrc.2019.08.014. Epub 2019 Aug 9. PMID: 31405561.
- Pingitore A., Iervasi G., Forini F. Role of the Thyroid System in the Dynamic Complex Network of Cardioprotection. Eur. Cardiol. 2016 Aug. 11(1). 36-42. doi: 10.15420/ecr.2016:9:2. PMID: 30310446; PMCID: PMC6159410.
- Seo S.M., Koh Y., Park H., Kim D.B., Her S.H., Lee J.M., et al. Thyroid stimulating hormone elevation as a predictor of long-term mortality in patients with acute myocardial infarction. Clin. Cardiol. 2018. 41. 1367-73. doi: 10.1002/clc.23062.
- Lee Y., Lim Y.H., Shin J.H., Park J., Shin J. Impact of subclinical hypothyroidism on clinical outcomes following percutaneous coronary intervention. Int. J. Cardiol. 2018. 253. 155-60. doi: 10.1016/j.ijcard.2017.09.192.
- Wang W., Wang S., Zhang K., Chen J., Zhang X., Shao C., et al. Hypothyroidism is associated with clinical outcomes in patients with acute myocardial infarction: subgroup analysis of China PEACE study. Endocrine. 2021. 74. 128-37. doi: 10.1007/s12020-021-02742-w.
- Inoue K., Ritz B., Brent G.A., Ebrahimi R., Rhee C.M., Leung A.M. Association of subclinical hypothyroidism and cardiovascular disease with mortality. JAMA Netw Open. 2020. 3. e1920745. doi: 10.1001/jamanetworkopen.2019.20745.
- Tsai T.Y., Tu Y.K., Munir K.M., Lin S.M., Chang R.H.E., Kao S.L., et al. Association of hypothyroidism and mortality in the elderly population: a systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2020. 105. dgz186. doi: 10.1210/clinem/dgz186.
- Wyne K.L., Nair L., Schneiderman C.P., Pinsky B., Antunez Flores O., Guo D., Barger B., Tessnow A.H. Hypothyroidism Prevalence in the United States: A Retrospective Study Combining National Health and Nutrition Examination Survey and Claims Data, 2009-2019. J. Endocr. Soc. 2022 Nov 10. 7(1). bvac172. doi: 10.1210/jendso/bvac172. PMID: 36466005; PMCID: PMC9706417.
- Song F., Bao C., Deng M., Xu H., Fan M., Paillard-Borg S., Xu W., Qi X. The prevalence and determinants of hypothyroidism in hospitalized patients with type 2 diabetes mellitus. Endocrine. 2017 Jan. 55(1). 179-185. doi: 10.1007/s12020-016-1095-2. Epub 2016 Sep 7. PMID: 27605039.
- Zhang M., Sara J.D.S., Matsuzawa Y., Gharib H., Bell M.R., Gulati R., et al. Clinical outcomes of patients with hypothyroidism undergoing percutaneous coronary intervention. Eur. Heart J. 2016. 37. 2055-65. doi: 10.1093/eurheartj/ehv737.
- Sampaolo G., Campanella N., Catozzo V., Ferretti M., Vichi G., Morosini P. Relationship between hypothyroidism and cholesterol out of the records of 1756 patients. Recenti Prog. Med. 2014 Feb. 105(2). 79-82. (Italian). doi: 10.1701/1417.15701. PMID: 24625905.
- Vale C., Neves J.S., von Hafe M., Borges-Canha M., Leite-Moreira A. The role of thyroid hormones in heart failure. Cardiovasc. Drugs Ther. 2019. 33. 179-88. doi: 10.1007/s10557-019-06870-4.
- Evron J.M., Hummel S.L., Reyes-Gastelum D., Hay–mart M.R., Banerjee M., Papaleontiou M. Association of thyroid hormone treatment intensity with cardiovascular mortality among US veterans. JAMA Netw Open. 2022. 5. e2211863. doi: 10.1001/jamanetworkopen.2022.11863.