
Журнал «Медицина неотложных состояний» Том 19, №3, 2023
Вернуться к номеру
Оцінка ефективності корекції крововтрати у постраждалих із проникними мінно-вибуховими травмами на етапі стабілізації та підготовки до аеромедичної евакуації
Авторы: Ухач Ю.Д.
Українська військово-медична академія, м. Київ, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
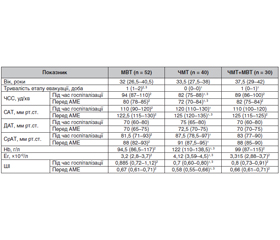
Стратегії лікування постраждалих із геморагічним шоком все ще є предметом наукового та клінічного інтересу, оскільки удосконалення підходів щодо швидкої та ефективної стабілізації постраждалих призведе до поліпшення виживання. Мета дослідження: порівняльна оцінка ефективності корекції крововтрати у постраждалих із проникними мінно-вибуховими травмами на етапі стабілізації та підготовки до аеромедичної евакуації (АМЕ). Матеріали та методи. У дослідженні ретроспективно за 3 роки (2016–2019 рр.) проаналізовано медичні карти 122 постраждалих, які отримали поранення під час виконання бойових завдань у районі проведення Антитерористичної операції/Операції об’єднаних сил. Постраждалих із бойовою травмою було розподілено на три групи. Усім постраждалим військовослужбовцям проводилася аеромедична евакуація гелікоптерами із польових госпіталів з метою переведення на етап надання спеціалізованої медичної допомоги. Ступінь шоку у постраждалих було визначено за допомогою методу арифметичного розрахунку шокового індексу (ШІ) Альговера та за даними лабораторних досліджень. Інфузійно-трансфузійна терапія на етапі стабілізації проводилася колоїдними та кристалоїдними розчинами, які при великих обсягах крововтрати доповнювалися переливанням свіжозамороженої плазми та еритроцитарної маси за традиційною схемою поповнення крововтрати на етапі надання медичної допомоги. Результати. У результаті проведення стабілізаційних заходів спостерігалося зниження ЧСС на 13,5 % (95% ДІ 11,2–15,7 %) на етапі підготовки до АМЕ. Спостерігалося зростання показника САТ у досліджуваних групах. Середній артеріальний тиск (СрАТ) у постраждалих із мінно-вибуховими торакоабдомінальними пораненнями під час госпіталізації становив 81,5 (71–93) мм рт.ст., а після проведення стабілізаційних заходів зріс до 88 (82–93) мм рт.ст. Встановлено вірогідну відмінність між групами мінно-вибухової та черепно-мозкової травми на етапах дослідження (p < 0,05). У результаті проведення стабілізаційних заходів вдалося знизити показники ШІ у досліджуваних групах на 23,7 % (95% ДІ 19,2–29,5 %). Висновки. Застосування комплексу стабілізаційних заходів у постраждалих із проникними мінно-вибуховими травмами на етапі госпіталізації дозволило поліпшити показники вітальних функцій та на 23,7 % (95% ДІ 19,2–29,5 %) знизити значення показників ШІ.
Management strategies in patients with hemorrhagic shock are still of scientific and clinical interest, as improved approaches to rapid and effective stabilization will lead to increased survival outcomes. The purpose of the study: to compare the effectiveness of blood loss correction in victims with penetrating blast injuries at the stage of stabilization and preparation for aeromedical evacuation. Materials and methods. The study retrospectively analyzed the medical records of 122 patients who were injured while performing combat missions in the area of the Anti-Terrorist Operation/Joint Forces Operation for 3 years (2016–2019). Victims with combat trauma were divided into three groups. All injured servicemen were evacuated by helicopters from field hospitals in order to transfer them to the stage of providing specialized medical care. The degree of shock was determined using Allgower’s method of arithmetic calculation of the shock index and according to the data of laboratory studies. Fluid therapy at the stage of stabilization was carried out with colloid and crystalloid solutions, which, in case of a massive blood loss, were supplemented by transfusion of the fresh frozen plasma and packed red blood cells according to the traditional scheme of replenishing blood loss at the stage of providing medical assistance. Results. As a result of stabilization measures, a decrease in heart rate by 13.5 % (95% confidence interval (CI) 11.2–15.7 %) was observed at the stage of preparation for aeromedical evacuation. An increase in systolic blood pressure was detected in the studied groups. The average blood pressure in victims with blast thoraco-abdominal injuries during hospitalization was 81.5 (71–93) mmHg, and after stabilization measures, it increased to 88 (82–93) mmHg. A significant difference was found between the groups of patients with blast trauma and traumatic brain injuries at the stages of the study (p < 0.05). As a result of stabilization measures, it was possible to reduce shock index in the studied groups by 23.7 % (95% CI 19.2–29.5 %). Conclusions. The use of a set of stabilization measures in patients with penetrating blast injuries at the stage of hospitalization made it possible to improve vital functions by 23.7 % (95% CI 19.2–29.5 %), and to reduce shock index.
мінно-вибухова травма; шоковий індекс; аеромедична евакуація
blast injury; shock index; aeromedical evacuation
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Spahn D.R., Bouillon B., Cerny V. et al. The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition. Crit. Care. 2019. 23. 98. https://doi.org/10.1186/s13054-019-2347-3.
- Caspers M., Maegele M., Fröhlich M. Current strategies for hemostatic control in acute trauma hemorrhage and trauma-induced coagulopathy. Expert Review of Hematology. 2018. 11. 12. 987995. https://doi.org/10.1080/17474086.2018.1548929.
- Schäfer N., Driessen A., Fröhlich M. et al. Diversity in clinical management and protocols for the treatment of major bleeding trauma patients across European level I Trauma Centres. Scand. J. Trauma Resusc Emerg. Med. 2015. 23. 74. https://doi.org/10.1186/s13049-015-0147-6.
- Kirkman E., Watts S. Haemodynamic changes in trauma. Br. J. Anaesth. 2014 Aug. 113(2). 266-75. doi: 10.1093/bja/aeu232. PMID: 25038158.
- Hinojosa-Laborde C., Hudson I.L., Ross E., Xiang L., Ryan K.L. Pathophysiology of Hemorrhage as It Relates to the War–fighter. Physiology (Bethesda, Md.). 2022. 37(3). 141-153. https://doi.org/10.1152/physiol.00028.2021.
- Xiang L., Calderon A. S., Klemcke H. G., Hinojosa-Labor–de C., Becerra S. C., Ryan K. L. A novel animal model to study delayed resuscitation following traumatic hemorrhage. Journal of Applied Physiology (Bethesda, Md.: 1985). 2022. 133(4). 814-821. https://doi.org/10.1152/japplphysiol.00335.2022.
- Strauss R., Menchetti I., Perrier L., Blondal E., Peng H., Sullivan-Kwantes W., et al. Evaluating the Tactical Combat Casualty Care principles in civilian and military settings: systematic review, knowledge gap analysis and recommendations for future research. Trauma Surgery & Acute Care Open. 2021. 6(1). E000773. https://Doi.Org/10.1136/Tsaco-2021-000773.
- Gurney J.M., Spinella P.C. Blood transfusion management in the severely bleeding military patient. Current Opinion In Anaesthesiology. 2018. 31(2). 207-214. https://doi.org/10.1097/ACO.0000000000000574.
- Kenney K., Amyot F., Haber M., Pronger A., Bogoslovsky T., Moore C., Diaz-Arrastia R. Cerebral Vascular Injury in Traumatic Brain Injury. Experimental Neurology. 2016. 275. Pt 3. 353-366. https://doi.org/10.1016/j.expneurol.2015.05.019.
- Leung L.Y., Deng-Bryant Y., Shear D., Tortella F. Combined hypoxemic and hypotensive insults altered physiological responses and neurofunction in a severity-dependent manner following penetrating ballistic-like brain injury in rats. J. Trauma Acute Care Surg. 2015 Oct. 79(4 Suppl. 2). S130-8. https://doi:10.1097/TA.0000000000000785. PMID: 26406425.
- Dennis A.M., Haselkorn M.L., Vagni V.A., Garman R.H., Janesko-Feldman K., Bayir H., et al. Hemorrhagic shock after experimental traumatic brain injury in mice: effect on neuronal death. Journal of Neurotrauma. 2009. 26(6). 889-899. https://doi.org/10.1089/neu.2008.0512.
- Hemerka J.N., Wu X., Dixon C.E., Garman R.H., Exo J.L., Shellington D.K., et al. Severe brief pressure-controlled hemorrhagic shock after traumatic brain injury exacerbates functional deficits and long-term neuropathological damage in mice. Journal of Neurotrauma. 2012. 29(12). 2192-2208. https://doi.org/10.1089/neu.2011.2303.
- Oley L.M., Iqbal O’Meara A.M., Wisniewski S.R., Hit–chens T.K., Melick J.A., Ho C., Jenkins L.W., Kochanek P.M. MRI assessment of cerebral blood flow after experimental traumatic brain injury combined with hemorrhagic shock in mice. Journal of cerebral blood flow and metabolism: official journal of the International Socie–ty of Cerebral Blood Flow and Metabolism. 2013. 33(1). 129-136. https://doi.org/10.1038/jcbfm.2012.145.
- Zusman B.E., Kochanek P.M., Bailey Z.S., Leung L.Y., Vagni V.A., Okonkwo D.O., et al. Multifaceted Benefit of Whole Blood Versus Lactated Ringer’s Resuscitation After Traumatic Brain Injury and Hemorrhagic Shock in Mice. Neurocritical Сare. 2021. 34(3). 781-794. https://doi.org/10.1007/s12028-020-01084-1.