
Журнал «Боль. Суставы. Позвоночник» 2 (18) 2015
Вернуться к номеру
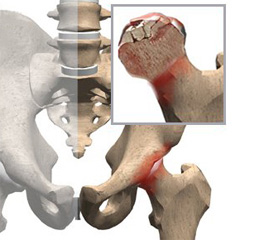
Aseptic Necrosis of the Femoral Head as a Possible Consequence of Hodgkin Lymphoma Chemotherapy
Авторы: Uglyar T., Zhulkevych I., Nedoshitko V. - Ternopil State Medical University named after I.Ya. Gorbachevsky, Ternopil, Ukraine
Рубрики: Ревматология, Травматология и ортопедия
Разделы: Медицинские форумы
Версия для печати
Статья опубликована на с. 97-98
Introduction. Four adult patients with malignant Hodgkin’s lymphoma were treated with combination chemotherapy including an alkylating agent and intermittent high–dose prednisone (in two cases). Twelve to 24 months after initiation of therapy, osteonecrosis of the femoral head developed. This was unilateral in all cases, and presumably didn’t represent a complication of steroid administration, as two of the patients received 4 and 6 month of corticosteroids therapy. Necrosis of bone may be a low–frequency long–term complication of combination chemotherapy in lymphoma.
Administration of corticosteroids is known to be associated with the development of osteonecrosis, or avascular necrosis of bone, particularly of the femoral and humeral heads. In the main, this occurs in patients receiving doses in excess of physiologic replacement for prolonged periods of time. In recent years, increasing numbers of patients with malignant Hodgkin’s lymphoma have been treated intermittently with combinations of chemotherapeutic agents, including corticosteroids.
Materials and methods. From 2009 through 2014, 283 patients were treated with chemotherapeutic regimens involving a combination of drugs for advanced Hodgkin’s disease. Virtually all the patients were adults. The treatment programs consisted of intermittent administration of such schemes of chemotherapy as ABVD and BEACOPP. Drug dosages and scheduling have been described in detail elsewhere, but the BEACOPP combination includes the administration of 2 weeks of daily oral prednisone, 40 mg/m2 body surface area for 4–6 month. All charts of these lymphoma patients in whom a diagnosis of aseptic or avascular necrosis of bone had been recorded (two patients both ABVD and BEACOPP) were reviewed for this report. In all instances the bone abnormality involved the femoral head and developed after initiation of chemotherapy. The diagnoses were made by radiographic means, using standard criteria, and operative intervention has been required and performed in all these patients.
Results. We wish to report the appearance of osteonecrosis in four such patients, two of whom were given 4 to 6 month of intermittent steroid therapy. These four cases of osteonecrosis arising after combination chemotherapy for lymphoma represent 1.4 % of all our patients so trea–ted. The time from initiation of corticosteroid (and additional cytotoxic) therapy to radiographic diagnosis of osteonecrosis was 12 and 16 months in the two patients in whom intermittent steroids were given. The other two patients, who hadn’t received intermittent steroids, in 12 and 24 months abnormal roentgenogram occurred. This was unilateral in all cases. All but one were male, despite an approximately unitary sex ratio in our patient population. The symptoms of hip and lower extremity pain were typical, the surgical intervention was considered and performed in all four patients.
Conclusion and discussion. Several theories have been proposed to account for an increased incidence of osteonecrosis after combined chemotherapy administration. Vascular obstruction by fatty emboli in areas of bone with poor collateral circulation is a mechanism that is often discussed, and both clinical and experimental supporting evidence have been described. These findings have not been confirmed by others, however; microtrauma in osteoporotic bone, possibly exacerbated by diminished sensibility from the antiinflammatory effects of steroids is among other suggested etiologic factors. Avascular necrosis of bone has complicated the treatment of a variety of diseases, including many in which this lesion is not part of the natural history of the disease. To our knowledge, osteonecrosis has previously been reported in the course of intermittent corticosteroid therapy of lymphoma, as well as in untreated lymphoma among the conditions associated with development of avascular necrosis of the femoral head. Steroids were administered to two of our patients for relatively long periods of time. In some reviews of the problem of aseptic necrosis complicating steroid therapy, the time from initiation of treatment to development of necrosis is stated to vary from 6 to 54 months. Daily prednisone dosage in most patients was 10–90 mg. Such articles point out that total steroid dose, daily dose, and duration of drug administration associated with osteonecrosis may be minimal. The possibility that our patients suffered from idiopathic necrosis of the femoral head should also be considered. This disease is reported to be rare but some authors think recognition of the entity is increasing. An increased incidence of the male sex, minor trauma, alcoholism, and hyperuricemia has been described in «idiopathic» cases. At least one of the latter three factors was questionably in all of our four patients. The importance, if any, in the development of bone necrosis of the cytotoxic drugs — an alkylating agent and vincristine in all instances, and procarbazine in two–administered to our patients — is yet unknown. We have assumed unlikely that the femoral head necrosis in our patients is related to the high dose but intermittent prednisone given in the combination chemotherapy protocols utilized in treatment of lymphoma. As the frequency of remission induction and disease–free survival of these patients improved long–term complications of intensive chemotherapy have become apparent. Osteonecrosis in a small percentage of intensively treated cases may be among these complications. And etiologic relationship of the corticosteroids to bone disease in such patients is uncertain.